12 Nov 2021
Golden rules of congestive heart failure – and case ‘walk-through’
Fiona Tomczynska and Dave Dickson use a patient example to describe how this clinical judgement aid is applied in the diagnosis of canine degenerative mitral valve disease.

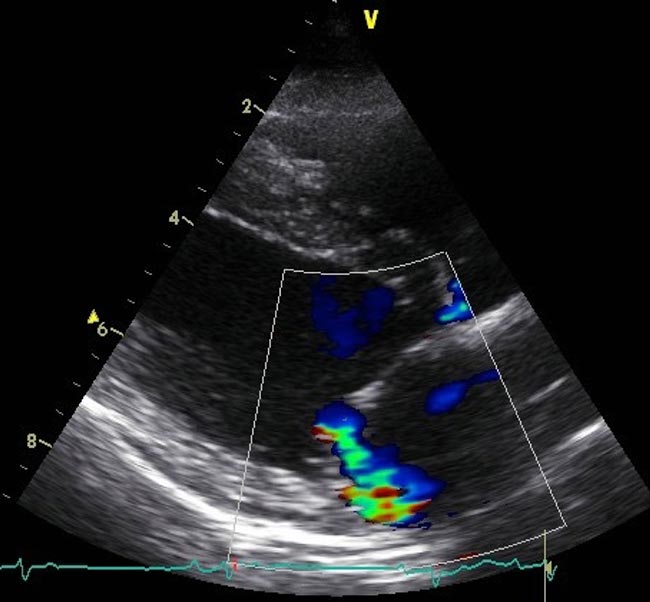
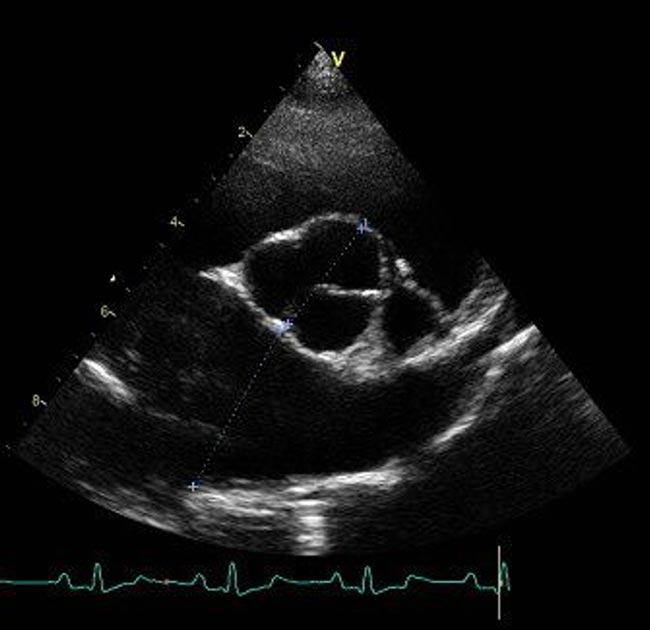
Figure 2. Right parasternal long-axis, four‑chamber view with colour flow Doppler showing a moderate mitral regurgitation jet projected towards the atrial free wall.
The golden rules are a guide for the management of small‑breed dogs with degenerative mitral valve disease (DMVD). They should be used to guide clinical decision‑making.
In the following case example, the authors explain how these rules can be applied in practice to the “everyday” case. The rules have been adapted from work by Mark Kittleson and Mark Rishniw of the Veterinary Information Network.
So, how can these rules be applied to a case example?
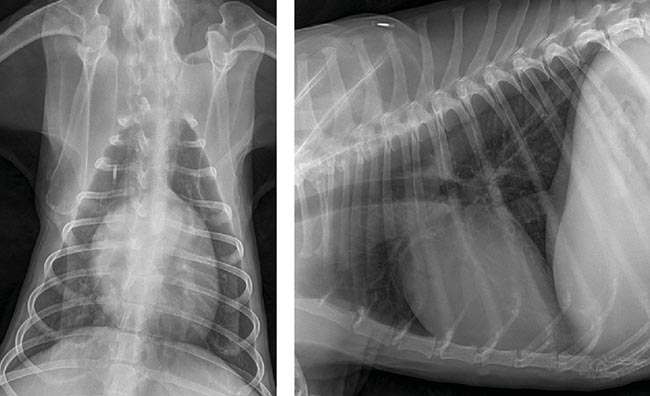
A 10-year-old neutered male Jack Russell terrier presented with a two-month history of coughing. The cough occurred initially when exercising, but progressed to occur randomly on an hourly basis.
The owner had not noticed any further breathing abnormalities, although the dog was panting more during and after walks. He showed no signs of lethargy, exercise intolerance or collapse. Vaccination and antiparasitic medications were up to date, with no history of travel outside the UK.
Physical examination
The patient was bright, alert and responsive, with a body condition score of 3/9 (weight 9.5kg). RR was slightly elevated at 32brpm and expiratory effort was mildly increased, with increased “crackle” lung sounds throughout the lung fields.
Heart rate was 132bpm in a regular rhythm, with a grade 4/6 systolic murmur heard loudest of the left apex and audible on the right.
Rectal temperature was 38.6°C and peripheral lymph nodes were normal on palpation. Mucous membranes were pink and capillary refill time was two seconds. A hacking non‑productive cough was elicited a few seconds after tracheal pinch. Abdominal palpation was normal.
| Table 1. Differential diagnoses of a progressive and non-productive cough | |
|---|---|
| Clinical sign | Differential diagnoses |
| Inflammation | Chronic bronchitis |
| Infection | Bordetellosis, Angiostrongylus vasorum, Oslerus Osleri, coccidioidomycosis |
| Miscellaneous | Aspiration pneumonia, idiopathic pulmonary fibrosis, inhaled foreign body, laryngeal paralysis, left atrial enlargement, primary ciliary dyskinesia |
| Neoplasia | Metastatic disease, alveolar carcinoma, adenocarcinoma, squamous cell carcinoma |
| Pulmonary haemorrhage | Coagulopathy, neoplasia, traumatic (A vasorum) |
| Pulmonary oedema | Cardiogenic, hypoproteinaemia, obstruction of lymphatic drainage |
Further investigations were carried out on this patient to determine the source of the cough, and a diagnosis of chronic bronchitis and DMVD stage B1 (ACVIM classification) was made.
This is a classic “everyday” example of how the “golden rules of CHF’ can be used to guide clinical decision-making in small-breed dogs with left‑sided heart disease.