15 Oct 2024
Rachel Carter and Emily Dutton discuss the latest on diagnosis and prognosis of this condition.

Image © Mikkel Bigandt / Adobe Stock

Image © Mikkel Bigandt / Adobe Stock
Degenerative valve disease (DVD) is the most common cardiac disease in dogs1 and is characterised by myxomatous degeneration of the valve and its chordae tendineae2,3, resulting in valvular regurgitation.
The mitral valve is most frequently affected, although the tricuspid valve is additionally affected in at least 30% of patients4. The aortic and pulmonic valves are more rarely affected (being affected alone in 2.1% and 0.4% of cases, respectively, and in some combination in 6.1% of cases5).
DVD is most prevalent in older, small-breed dogs6-8. Larger dogs may sometimes also be affected and tend to exhibit faster disease progression with more apparent systolic dysfunction9,10. Cavalier King Charles spaniels (CKCS) may sometimes be affected at a younger age and, anecdotally, seem to experience faster disease progression when this is the case.
DVD is typically slowly progressive and may well not progress within the patient’s lifetime to cause clinical signs9,11. In some dogs, however, volume loading imposed by the mitral regurgitation leads to progressive left-sided cardiomegaly and subsequent left-sided congestive heart failure (CHF)11,12.
As such, a staging scheme has been developed to categorise dogs according to their place in the disease time course9:
● Stage A. Describes dogs which are of a predisposed breed (such as the CKCS), but do not currently have valve changes consistent with DVD.
● Stage B. Describes dogs with valve changes and regurgitation consistent with DVD, but which have never developed CHF. Stage B is further divided into stage B1 and stage B2.
■ Stage B1. Describes dogs without left-sided cardiomegaly (or without changes sufficient to meet the criteria for stage B2).
■ Stage B2. Describes dogs with left-sided cardiomegaly that meets specific criteria (discussed further later in this article).
● Stage C. Describes dogs with CHF due to their DVD, which may either be causing clinical signs or may currently be controlled with medications.
● Stage D. Describes dogs with CHF refractory to standard treatment.
This article will discuss the diagnosis of DVD in dogs, both with and without clinical signs of CHF. It will also discuss factors that may be used to help evaluate prognosis. These areas will be discussed in the context of first opinion practice, in which full echocardiography may not be available for all patients.
DVD is most commonly suspected when a murmur typical of mitral regurgitation – that is, a left apical systolic murmur – is detected incidentally9. In some dogs, clinical signs of CHF may not develop for years following murmur detection, if at all11,12.
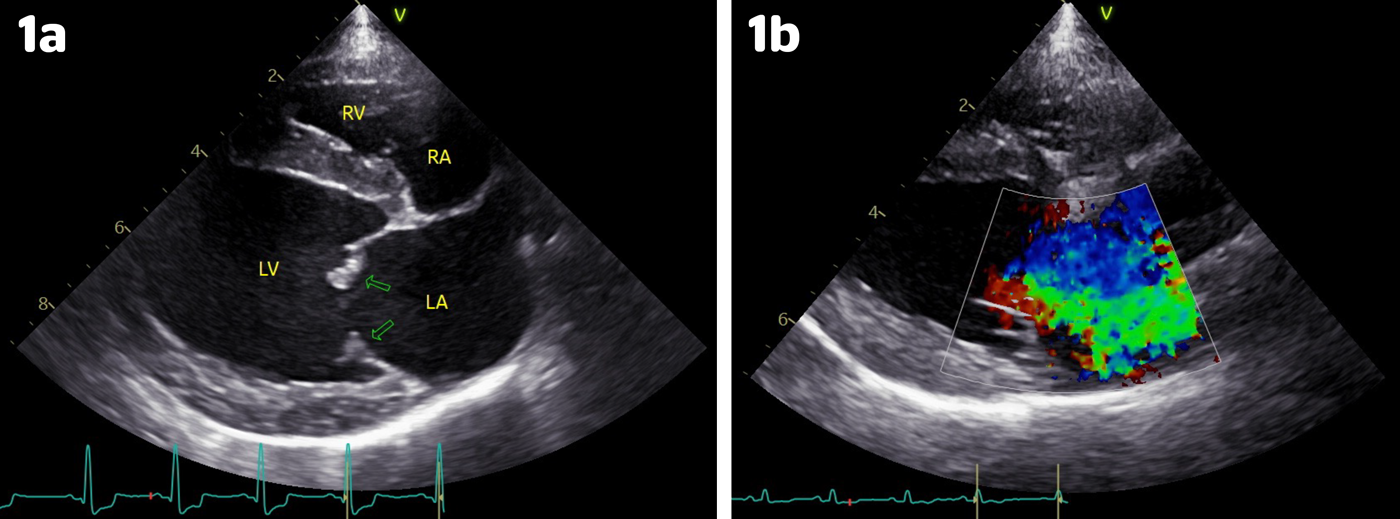
Figure 1. Right parasternal long axis four-chamber echocardiographic views taken from dogs with degenerative valve disease documenting (Figure 1a) thickened and nodular mitral valve leaflets (green arrows) and (Figure 1b) mitral valve regurgitation (green flow) identified using colour Doppler. LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle.
Arguably, more important than diagnosis of DVD as a whole is the diagnosis of stage B2 DVD. This is because the EPIC study (Boswood et al, 2016) showed that pimobendan treatment initiated in stage B2 DVD delayed the onset of CHF or cardiac-related death by an average of 15 months14. In this study, dogs in stage B2 took an average of two years and one month to develop CHF or experience cardiac-related death without pimobendan treatment, but an average of three years and four months with pimobendan treatment. Echocardiographic evidence of both left atrial and left ventricular enlargement – that is, a left atrial to aortic root ratio (LA/Ao) greater than or equal to 1.6, and a bodyweight normalised left ventricular internal diameter in diastole (LVIDDN) greater than or equal to 1.7 – is required for the diagnosis of stage B2 (Figure 2).
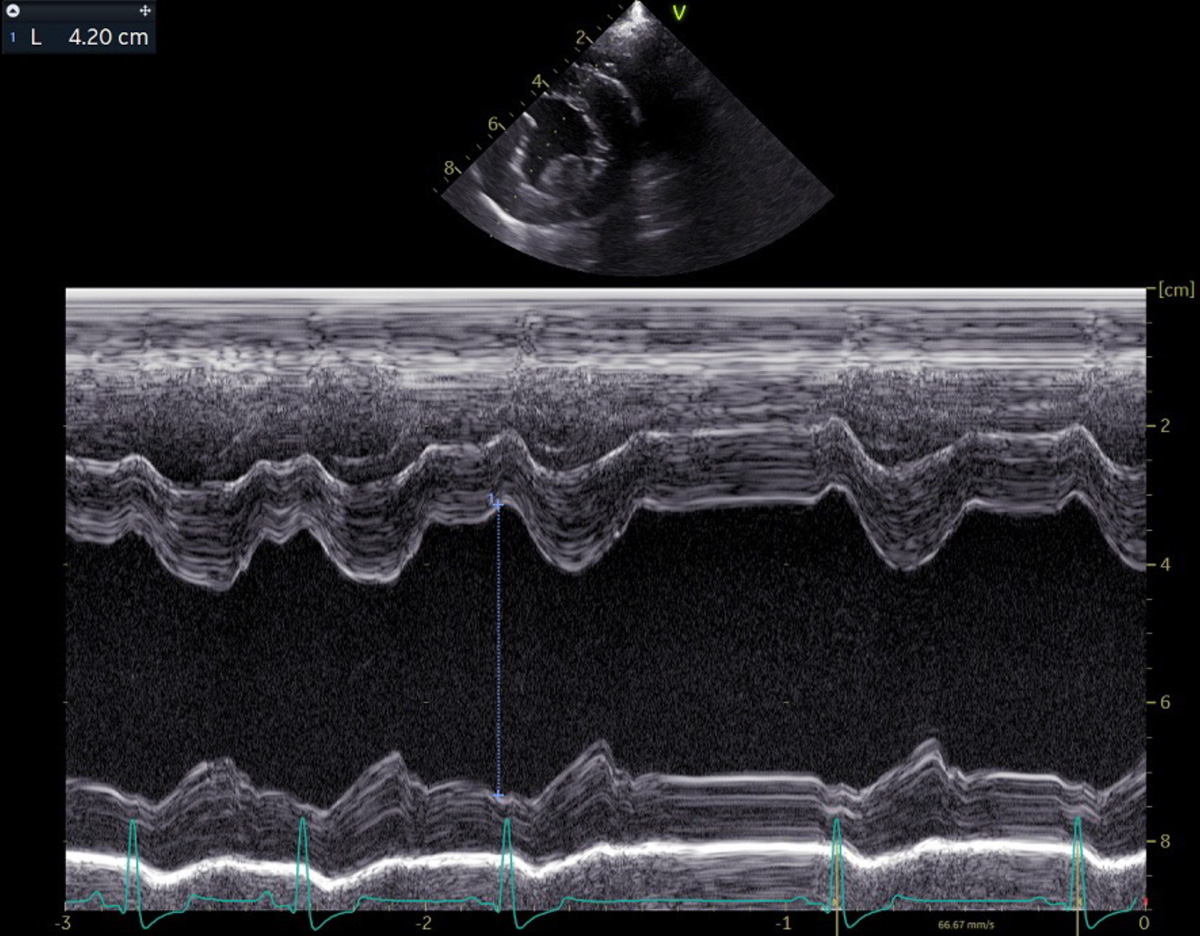
Figure 2a. An M-mode from a right parasternal short-axis echocardiographic view at the level of the papillary muscles, demonstrating measurement of the left ventricular internal diameter in diastole, which is measured at the start of the QRS complex.
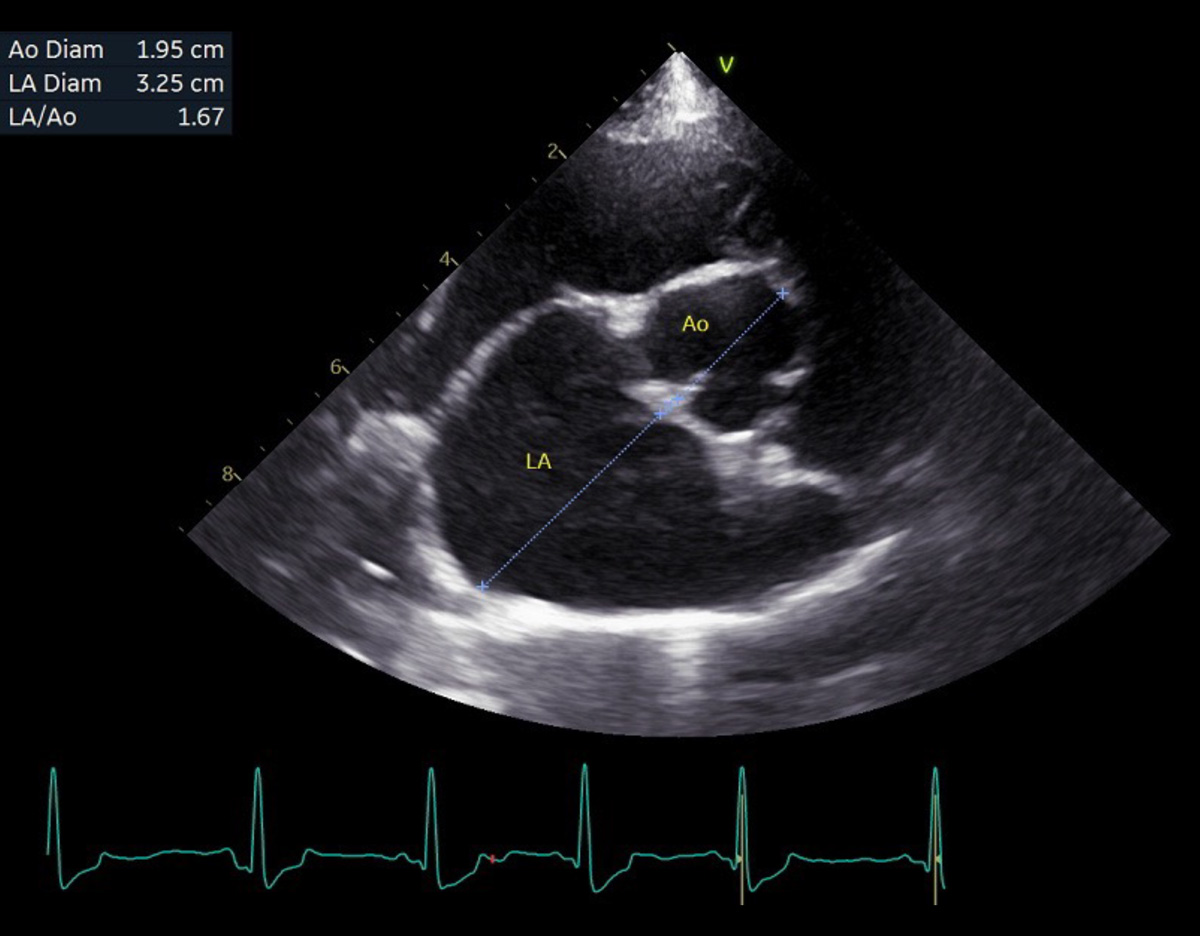
Figure 2b. A right parasternal short-axis echocardiographic view at the level of the aortic valve, demonstrating measurement of the left atrial to aortic root ratio (LA/Ao), which is measured immediately following aortic valve closure. Ao = aorta; LA = left atrium.
The American College of Veterinary Internal Medicine 2019 mitral valve disease consensus statement9 proposed that clear evidence of cardiac enlargement on thoracic radiographs may potentially be used as a substitute for echocardiography in the diagnosis of stage B2 DVD, where echocardiography was unavailable. Proposed cut-off values for stage B2 were a vertebral heart score (VHS) of greater than or equal to 11.5, a VHS greater than the breed-specific reference range where one was available, a vertebral left atrial size (VLAS) greater than or equal to 3, or a faster rate of increase in cardiac size compared to previous years if yearly radiographs had been taken (Figure 3).

Figure 3. A right lateral thoracic radiograph of dog depicting measurement of (Figure 3a) vertebral heart score (VHS) and (Figure 3b) vertebral left atrial size (VLAS). VHS is measured by extending a line from the ventral aspect of the carina to the cardiac apex, and another line perpendicular to the first at the widest point of the cardiac silhouette. Both lines are compared to the vertebral bodies, starting at the cranial edge of T4. The number of vertebral bodies is then added together to give the VHS (in this case, 5.9 plus 5.1 equals 11.0). The VLAS is measured by extending a line from the ventral aspect of the carina to where the dorsal border of the caudal vena cava intersects the left atrium. The line is compared to the vertebral bodies, starting at the cranial edge of T4 (in this case, VLAS equals 2.2).
Subsequent studies have shown conflicting results as to the best radiographic measurement to use for identifying stage B2, with VLAS15,16, VHS17 and radiographic left atrial dimension (RLAD)18 all being reported as most useful by different studies. For VLAS, cut-off values ranging from greater than or equal to 2.3 to greater than or equal to 2.6 have been found to give the highest combined sensitivity and specificity for identifying stage B2, while values ranging from greater than or equal to 2.4 to greater than or equal to 3.1 have been reported to maximise specificity (lowest chance of false positives)15,16,18-20.
For VHS, cut-off values ranging from greater than or equal to 10.7 to greater than or equal to 12 have been found to give the highest combined sensitivity and specificity, while values ranging from greater than or equal to 11.6 to greater than or equal to 12.25 have been reported to maximise specificity15-19.
Echocardiography remains the gold standard for identifying stage B2 DVD, since a large-scale study has shown that thoracic radiography can give both false positive and false negative results when detecting cardiomegaly in dogs with DVD21. One study found a VHS cut-off of greater than 10.8 to provide few false negatives when identifying stage B2, and a cut-off of greater than 11.7 to provide few false positives. However, more than 40% of the dogs in this study had a VHS between these two values17.
One study assessed the possibility of using a combination of history, physical examination and blood testing to identify stage B2 degenerative mitral valve disease (DMVD)22, and found that dogs with elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP) concentrations, higher murmur grades, reduced appetites, reduced body condition scores (less than or equal to 3 out of 9), higher serum alanine aminotransferase concentrations and lower serum creatinine concentrations were more likely to be in stage B2 (versus stage B1 DMVD). Circulating NT-proBNP concentrations and murmur grade were the most important predictors for stage B2 DMVD.
Another study looked at predicting stage B2 specifically in CKCSs. Murmur grade, VHS (which slightly outperformed VLAS in this study) and NT-proBNP were important predictors of stage B2, and the study authors provided a decision tree to help distinguish CKCSs in stage B2 from those in stages B1 and A23. Ideally, the results of these two studies should be used to encourage echocardiography in dogs considered to be at higher risk for stage B2, rather than to definitively diagnose stage B2 (without using echocardiography). It is worth noting that, in one of the studies, no stage B2 dogs had a murmur quieter than grade III/VI23 and, in the other, only 4.5% of the B2 dogs had a murmur quieter than grade III/VI22.
Thus, where the cost of repeated echocardiograms is unlikely to be feasible, a veterinarian can have fair confidence in foregoing echocardiographic examination while the murmur is still grade I/VI or grade II/VI.
Clinical signs of left-sided CHF include tachypnoea, dyspnoea, restlessness or coughing9. In the patient with CHF due to DVD, thoracic radiography should demonstrate a lung pattern consistent with cardiogenic pulmonary oedema, namely an interstitial to alveolar lung pattern with a peri-hilar, caudodorsal or diffuse distribution, as well as radiographic signs of cardiomegaly, left atrial enlargement and pulmonary venous congestion. Typically, the cranial lobar pulmonary veins are considered enlarged if they are wider than the proximal third of the fourth rib (best evaluated on lateral thoracic radiographs), and the caudal lobar pulmonary veins if they are wider than the ninth rib where they cross it (best evaluated on dorsoventral radiographs)24,25. Additionally, the pulmonary veins may be considered enlarged if they are wider than their corresponding arteries.
Evaluation of left atrial size via focused echocardiography, most commonly via measurement of LA/Ao, is extremely useful, as the left atrial size should be increased in almost all cases of CHF due to DVD (a rare exception being major chordae tendinae rupture where the left atrium has not yet had time to dilate). B-lines will likely be detected on point of care lung ultrasonography26.
Full echocardiography, where possible, is useful, as it allows further confirmation of CHF (through identification of indicators of increased left atrial pressure), definitive diagnosis of the DVD, and detection of complicating factors such as pulmonary hypertension. Sedation with butorphanol at 0.2mg/kg to 0.3mg/kg IM or IV may be used to facilitate investigations in stressed patients; however, some patients may only be stable enough for minimal investigation (such as assessment of LA/Ao and for B-lines in a standing position).
Challenges arise due to the fact that older, small-breed dogs with a respiratory cause for their tachypnoea or dyspnoea may have concurrent DVD, and so may have a heart murmur despite DVD not being the cause of their clinical signs. In dogs with normal or only mildly increased left atrial size, left-sided CHF is unlikely to be the cause of the tachypnoea and/or dyspnoea.
The ability to accurately assess LA/Ao is, therefore, very helpful. A lung pattern inconsistent with cardiogenic pulmonary oedema (for example, a bronchial pattern or pulmonary nodules) suggests a respiratory cause; however, alveolar and interstitial lung patterns may be seen with respiratory disease, as well as with left-sided CHF. Measuring VLAS may be used to help assess left atrial size and, therefore, may help distinguish between cardiogenic and non-cardiogenic causes of the clinical signs where focused or full echocardiography is unavailable.
One study found that, for older (older than or equal to 6 years old) small-breed (less than or equal to 20kg) dogs with clinical signs (defined in the study as tachypnoea in combination with dyspnoea, syncope and/or acute onset or worsening of coughing) and with a radiographic lung pattern potentially suggestive of pulmonary oedema, a VLAS of more than 2.5 was useful for identifying cases of CHF rather than respiratory disease27.

Image © otsphoto / Adobe Stock
A newer radiographic method of measuring left atrial size, the modified-VLAS, is both sensitive and specific for detecting echocardiographic left atrial enlargement28, although its accuracy specifically in identifying CHF has not yet been determined. Physical examination factors should be used to help assess the patient, as quieter murmurs reduce the likelihood of CHF and louder murmurs increase it27.
Additionally, a dog with a relatively low heart rate and sinus arrhythmia is unlikely to be in CHF9, since high sympathetic and low parasympathetic tone is expected in CHF cases. Thoracic ultrasonography (performed in sternal recumbency) is likely safer than thoracic radiography in unstable patients, and detection of numerous B-lines (more than three B-lines for at least two out of four anatomic sites for each haemithorax) showed similar diagnostic accuracy to thoracic radiography for detecting cardiogenic pulmonary oedema in one study26. However, B-line assessment was not useful in distinguishing cardiogenic pulmonary oedema from diffuse interstitial or alveolar respiratory disease (both result in multiple B-lines)26. The usefulness of NT-proBNP in distinguishing cardiac from non-cardiac causes of tachypnoea or dyspnoea may be limited by the time taken to receive the results.
Importantly, the presence of coughing alone (in the absence of other clinical signs such as tachypnoea or dyspnoea) in a dog with DVD may well not represent CHF, and instead might result from compression of the left mainstem bronchus by left atrial dilation and/or from concurrent respiratory disease. A furosemide trial in such cases may result in some improvement in the cough despite the absence of CHF, since furosemide has anti-inflammatory and bronchodilatory properties in addition to its diuretic effects29,30. This may lead to furosemide being given long term to dogs in which its use is not yet warranted.
Thoracic radiography can be used in coughing dogs with DVD to assess for the presence of left atrial dilation and elevation of the trachea and/or left mainstem bronchus, pulmonary oedema (indicating left-sided CHF), and concurrent respiratory disease. Additionally, the patient’s sleeping respiratory rate (SRR) should be monitored by the owner at home, as SRRs of less than 30 breaths per minute are unlikely to be consistent with the presence of CHF31,32. In fact, long-term SRR monitoring is used by many cardiologists as a means of helping detect the onset of stage C in patients with DVD, as a consistent increase in SRR to more than 30 breaths per minute likely indicates the onset of left-sided CHF and warrants diuretic therapy.
One study found that respiratory rate on physical examination was a predictor of the presence of CHF in dogs with DVD33. Other studies have found that an at-home SRR of more than 40 breaths per minute is the best predictor (superior to echocardiographic measurements) of uncontrolled left-sided CHF in patients undergoing CHF treatment34, and that dogs with medically well-controlled left-sided CHF are unlikely to have a SRR of more than 30 breaths per minute35. An increase in SRR may occur prior to the patient becoming dyspnoeic, thus reducing patient suffering if diuretic therapy is initiated or escalated. A normal NT-proBNP (less than 900pmol/L)36 result in a coughing dog makes CHF unlikely37. A VHS of less than or equal to 11.4 has been shown to have fair accuracy for excluding a cough being of cardiac origin (whether due to cardiac enlargement or CHF) in patients with DMVD38.
Syncope in dogs with DVD may be caused by factors such as pulmonary hypertension or an arrhythmia. Therefore, where syncope is present, referral for a full cardiac work-up is advised if at all possible.
As would be expected according to the DVD staging scheme, multiple studies have documented a poorer prognosis with increased left heart size. Specifically, increased mortality has been associated with a greater LA/Ao39, an LA/Ao greater than 1.711, a greater LVIDDN40,41 an LVIDD greater than 1.7940 and a greater VHS42. For asymptomatic dogs, an increased risk of CHF has been associated with a greater LA/Ao, a greater left ventricular size and a VHS greater than 1243. In stage B2, the risk of CHF or cardiac death is heightened with increasing LVIDDN44. Even if only patients already in CHF are considered, greater left atrial size45,46 and greater VHS45 are associated with a poorer outcome.
It has been shown in CKCSs that the left heart size (whether measured via echocardiography or thoracic radiography) tends to increase at a steady rate before rapidly increasing in the 6 to 12 months prior to the onset of CHF47,48. Therefore, if thoracic radiography is undertaken regularly, a more rapid rate of VHS increase can help to predict the onset of CHF within the next year48.
More in-depth echocardiographic analysis can also help to predict prognosis; for example, one study showed that greater severity of mitral valve prolapse or the presence of mitral valve flail (which indicates major chordae tendinae rupture) is associated with increased cardiac mortality49.
Increased mitral E wave velocity, which suggests increased left atrial pressure, is a particularly important negative prognostic indicator11,39,49,50; a mitral E wave velocity of more than 1.2m/s to more than 1.4m/s indicates a higher risk of mortality11,49,50. An echocardiographic scoring system (the MINE scoring system), which combines several echocardiographic factors (LA/Ao, LVIDDN, mitral E wave velocity and fractional shortening) has been developed, and has been shown to be associated with survival time, both between and within different DVD stages39 (the scoring system has recently been updated to include only LA/Ao, LVIDDN and mitral E wave velocity51).
Not unexpectedly, dogs with clinical signs of DVD (such as syncope, coughing, exercise intolerance or dyspnoea) have a greater risk of mortality11,40,42,52,53 compared to those without. Diuretic administration and dosage have also been linked to prognosis, likely due to being surrogate markers for the presence and severity of CHF46,52. Higher heart rates are associated with increased risk of CHF onset or cardiac death in dogs with stage B2 DMVD44 and with increased mortality in dogs with DMVD as a whole52. Older dogs, female dogs, CKCSs, purebred dogs, dogs weighing more than or equal to 20kg and dogs with louder murmurs (for example, murmur grade greater than III/VI) have been documented to have a worse prognosis in previous studies41,52-54. A reduced appetite and the absence of sinus arrhythmia have also been reported as poor prognostic indicators53.
Lastly, cardiac biomarkers may be used to help evaluate prognosis. Higher circulating NT-proBNP40,52 and high-sensitivity cardiac troponin I (hs-cTNI)41,52 concentrations have been associated with increased mortality in dogs with DMVD. A circulating NT-proBNP concentration of more than 1500pmol/L has been associated with an increased risk of developing CHF in dogs with asymptomatic DMVD43. In one study, survival time was shortest for dogs in which both NT-proBNP and hs-cTNI were elevated41.
This article has provided a summary of the diagnosis and prognostication of DVD in dogs. Determination of DVD stage can, in some instances, be challenging; however, this article has provided a summary of the different diagnostic techniques that may be used depending upon which are available to the attending clinician.
Determination of prognosis is important for owners of dogs with DVD. It may also become increasingly important should surgical or interventional mitral valve repair techniques become more widely available, since estimation of prognosis may be used to help select patients for which these procedures are likely to be of benefit.
Emily Dutton
Job TitleRachel Carter
Job Title