13 Aug 2024
BRD: impact on herds and improving vet involvement
While it remains a common and costly disease, many farmers are still reluctant to seek help with respiratory disease issues in their herds.
Phil Elkins
Job Title
Image © Syda Productions / Adobe Stock
Bovine respiratory disease (BRD) remains one of the most common disease complexes identified in UK calves, despite many decades of research into prevention and control of respiratory infections.
A cohort study of dairy farms using a standardised scoring system to identify calves with respiratory disease (and scour) found that 45.9% of calves succumbed to BRD (farm range 20.4% to 77.8%)1.
While the direct treatment costs are obvious – with medicine costs, labour and case fatalities in particular – the indirect costs, particular of mild cases, may not be as clear to producers or veterinary surgeons.
Animals with any degree of lung consolidation, as identified by thoracic ultrasound scanning as calves, have a 15% reduction in average daily liveweight gain2, and it is also associated with a reduction in first lactation milk production of 525kg3. This is obviously significant, but is exacerbated by the fact that heifers diagnosed with BRD are 2.85 times more likely to die and 2.3 times more likely to be removed from the herd before first calving4.
Yet despite the clear financial incentives to improve control of BRD, it remains highly prevalent. When considering the reasons why progress is not being made, it is important to firstly look at the disease from the viewpoint of the producer.
Farmers’ attitudes
A survey of farmers’ attitudes towards youngstock disease provides useful insights into the hurdles vets face with controlling BRD5. Perhaps most telling is the stage at which producers of different classes would engage their vet for advice regarding respiratory disease (Figure 1).
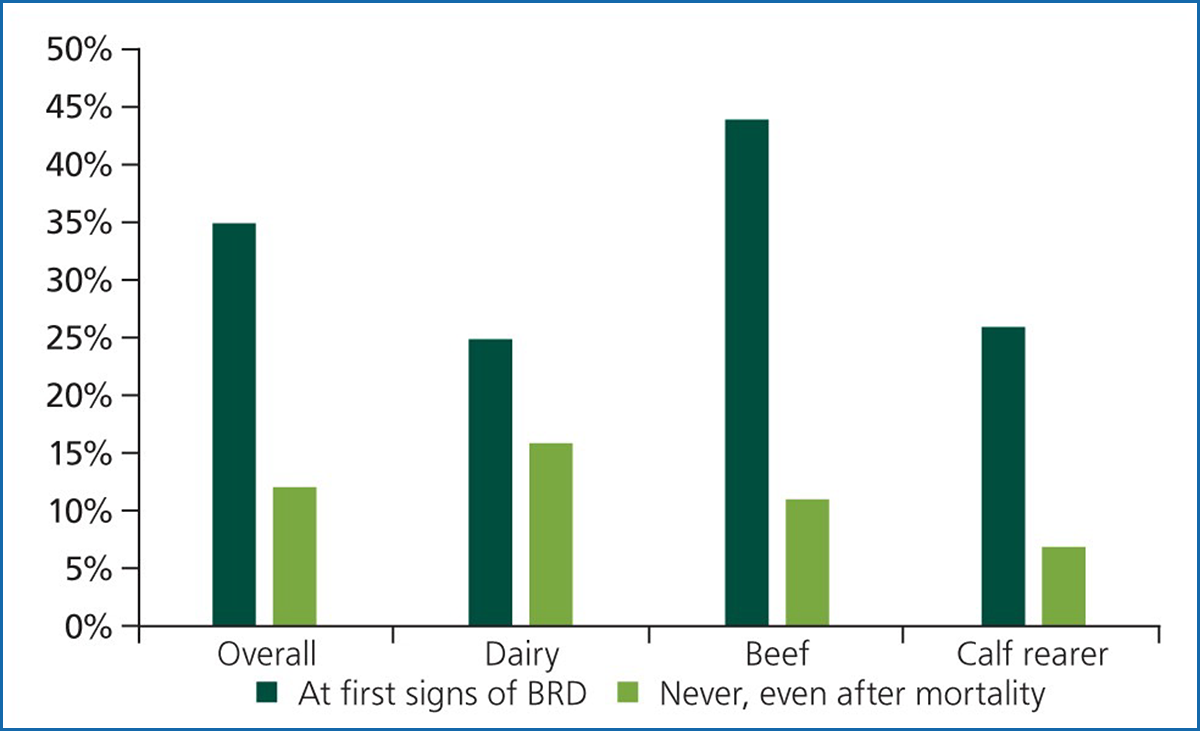
As can be seen, 12% of farmers reported they would never call out a vet for BRD, even after mortalities have been experienced. This is even more stark with dairy farmers, where more than 15% would never call out a vet. At the other extreme, 45% of beef farmers would ring a vet at the first signs of BRD.
This disconnect between vets and calf health extends even further. Diagnostics and vaccines can play a major role in reducing the impacts of BRD. However, the correct implementation of vaccines is dependent on appropriate diagnostics. Meanwhile, 66% of farmers use no diagnostics for respiratory disease at all.
Without knowing the pathogen profile on farm, how can a vet responsibly prescribe a vaccine for BRD? Many subsidised schemes are available from pharmaceutical companies for diagnostic testing for BRD, covering a range of pathogens and testing modalities. Worryingly, only 30% of farmers responded that they would change vaccine regime based on the results of diagnostics.
So, summarising the current situation, a disease complex exists affecting nearly 50% of all youngstock, affecting growth rate, production and retention within the herd, and for which many farmers would not consult their vet, do not test and would not change vaccine regime based on the results of the test. This represents both a significant weakness in the provision of health advice to farmers and a great opportunity for increased veterinary involvement for the benefit of both practice and client.
However, this suggests that if vets wait to be engaged regarding youngstock health, it may never happen – so proactivity is key.
Often, farmers will not recognise the extent of a BRD problem on their farm. For those with little or no historic veterinary involvement with BRD, a check of records will indicate the rate of clinical BRD and calf mortality. For many farms, even reliable treatment records may be absent – despite being a legal requirement. In this case, a review of medicine sales to the farm, and some creative extrapolation of data, will give a rough treatment rate.
Targets are published for respiratory disease and calf mortality; the skill of a vet health advisor is to use these targets together with an understanding of the farm practices to derive an expected or appropriate level of BRD. For example, a closed suckler herd with a targeted vaccine strategy, excellent housing and good stockmanship would expect to have a lower rate of BRD than a calf rearer sourcing from multiple markets with multiple suppliers, and with buildings with poor ventilation or draining.
That is not to say high rates of BRD are acceptable, more that what is achievable on individual units varies without significant management changes or investment.
Comparing the farm treatment and mortality levels with the expected level of disease on that or similar units – or, more importantly, the expected level of disease with achievable improvements – offers an opportunity to increase involvement in BRD control.
While the aforementioned prevalence is based on thoracic ultrasound scanning, treatment records indicate a rate of clinical BRD of between 11% and 16%.
On-farm studies showed an untreated rate of BRD (subclinical) of between 23% and 67%. It is possible to demonstrate the consolidation to farmers with thoracic ultrasound scanning, which, in the author’s experience, can be quite striking in animals with no clinical history.
Correlating these with current or future performance can then reinforce the need for change. Current performance is often hard to gauge, and in the absence of regular weight data, a weight or condition for age may be all that is available.
Identifying and quantifying the extent of subclinical infection can be a trigger for further veterinary involvement in BRD control. In many cases, identifying the current level of disease and consequences of disease are all a vet needs to engage with farmers on BRD, and a few targeted interventions can lead to large rewards, allowing more in-depth discussions as farmers move their mentality from BRD treatment (or apparent BRD acceptance in some circumstances) to BRD control.
Tools for diagnosis
A number of tools are available to improve the early identification of BRD and increase diagnosis of those subclinical (or less clinically obvious) cases contributing to disease losses.
Two scoring systems – the University of Wisconsin-developed calf health scoring system and the BRD scoring system from the University of California, Davis – have been described.
These are objective systems based on the identification of the clinical signs associated with BRD, with the aim of being performed regularly by calf-rearing staff, with a binary cut off for treatment – scores above × indicates BRD. These schemes have incredibly similar performance as a diagnostic test:
- screening sensitivity (for all respiratory disease): 46%
- diagnostic sensitivity (for “clinical” cases): 71% to 73%
- specificity: 87% to 91%6

As an on-farm screening tool to identify animals with disease, these are a significant improvement on current staff diagnosis. Training staff members on how to use these scoring systems and implement them into daily routines can prove incredibly useful at diagnosing disease early – and ensuring prompt, effective treatment.
Thoracic ultrasound scanning is a more involved procedure. However, once proficient, practitioners can quickly and effectively perform this at a regular vet visit. Offering this as a regular service can improve client education, while demonstrating and evidencing the impact of BRD in pre-weaned dairy calves.
Routine, strategic scanning demonstrates trends in new infection rate, cure rates and severity of lesions in those affected. Using the data to establish benchmarks for individual farms can allow prudent, evidence-based decisions on treatment and management changes to aid in prevention7. While quick scanning requires a learning period, many practitioners can achieve good accuracy, and it can be improved by skilled operator practical training8.
The uptake of technology on farm is increasing, with opportunities for increased diagnostic sensitivity for BRD. This is broadly split into two categories: behavioural analysis and physiological analysis. Behavioural analysis includes parameters such as feeding behaviour – quantity, frequency and timing – from automated calf feeding machines, and movement/activity through technology incorporating accelerometers.
Physiological analysis primarily focuses on temperature identification through either peripheral or external (infrared) sensors or internal (reticular) sensors in boluses.
Limited published evidence is available on the accuracy of these technologies, but what is available is very promising, with high sensitivities and specificities for identifying sick animals, often one to seven days before clinical signs develop9.
Treatment outcomes
Early treatment of disease would logically lead to better treatment outcomes and that is borne out in the evidence. On calves examined twice-weekly by experienced practitioners using both a standardised scoring system and ultrasound scanning, comparing tulathromycin treatment with a placebo on early cases led to a reduction in re-treatments within seven days and mortality, with an increase in growth rates.
However, irrelevant of whether the animals were treated with antibiotics, all calves that received even a single diagnosis of BRD entered the weaning phase with signs of pneumonia indicating that prompt treatment leads to a short-term improvement, but long-term damage remains10. This study did not use NSAIDs due to a lack of options regarding NSAID use in the US. Further work is needed on the benefits of early treatment of calves with BRD with NSAIDs, either in combination with antimicrobials or in isolation.
The old adage that prevention is better than cure is true of BRD, with remaining chronic damage affecting future performance. Environmental improvement must form the primary focus of BRD prevention, but due to the wide-ranging facilities and conditions on farms in the UK, a full review of environmental assessment is out of the scope of this article. It is also a widely reported subject in this and other publications.
Similarly, colostrum uptake continues to be variable, with more than 20% of calves demonstrating failure of passive transfer1. Again, this needs to be together with measures to ensure colostrum uptake is widely reported.
Vaccination as an adjunct to environmental optimisation is a key tool in the box for vets looking to improve control of BRD on farm. Unlike antimicrobials, for which the range is unlikely to expand in the near future, with increasing restrictions on use and categories available on a number of farms, the future in the vaccine market looks strong.
An increasing number of products are available, from a wide range of pharmaceutical suppliers, covering an increasing range of pathogens. Vaccines have been licensed for cover against bovine coronavirus and Mycoplasma bovis, and relatively recently a range of multivalent and monovalent vaccines have strengthened the offering to the veterinary market. This allows more in-depth conversations regarding vaccine uptake on farm.
The following are a few of the author’s thoughts with regards to vaccine use on farm:
● The absence of diagnostics makes vaccine success down to luck. Using the aforementioned subsidised schemes can increase the likelihood of vaccine success.
● Pay attention to timing. Consider the age at which animals succumb to BRD and ensure your vaccine choice will cover that period. If no vaccine is available for the pathogens present at the age desired, consider speaking to your technical vet from the pharmaceutical company regarding off-label use. This may include vaccinating dams to boost colostrum. Vaccines also do not work instantly – check the published onset of immunity.
● Ensure vaccines are stored appropriately. Periodically, check the temperatures in your client’s fridges.
● Vaccines boost immunity. They do not prevent infection. Reducing infection pressure is key to disease control, but vaccines will reduce the severity of any infection. This means fewer diseased (as not all infections lead to disease), lower severity, less mortality and fewer consequential losses. It does not mean no disease. If this is not explained to clients, the vaccine will never meet their expectations. The published literature for each vaccine will give a good guide as to expected improvements.
● Vaccines rely on a functioning immune system. If this is hampered by concurrent disease, malnutrition, poor colostrum intakes or any other factor, the vaccines will have limited impact. The other issues are more pressing and need fixing first.
In summary, BRD is still a major cause of both morbidity and mortality in calves, with limited veterinary involvement, limited uptake of diagnostics and a disconnect between vets and producers.
Some targeted interventions using record analysis and thoracic ultrasound scanning can allow quantification and monitoring of the issue at a farm level. Training in standardised scoring systems, or regular, practitioner-performed scanning can lead to improved detection, and prompt, effective treatment.
However, any disease, even if treated promptly, will lead to reduced future performance. Prevention of disease through improving the environment and ensuring optimum immunity is essential, but diagnostics and an appropriate vaccine regime can be a rewarding tool to improve control.
References
- Johnson KF, Chancellor N and Wathes DC (2021). A cohort study risk factor analysis for endemic disease in pre-weaned dairy heifer calves, Animals 11(2): 378.
- Cramer MC and Ollivett TL (2019). Growth of preweaned, group-housed dairy calves diagnosed with respiratory disease using clinical respiratory scoring and thoracic ultrasound – a cohort study, Journal of Dairy Science 102(5): 4,322-4,331.
- Dunn TR, Ollivett TL, Renaud DL, Leslie KE, LeBlanc SJ, Duffield TF and Kelton DF (2018). The effect of lung consolidation, as determined by ultrasonography, on first-lactation milk production in Holstein dairy calves, Journal of Dairy Science 101(6): 5,404-5,410.
- Buczinski S, Achard D and Timsit E (2021). Effects of calfhood respiratory disease on health and performance of dairy cattle: a systematic review and meta-analysis, Journal of Dairy Science 104(7): 8,214-8,227.
- Baxter-Smith K and Simpson R (2020). Insights into UK farmers’ attitudes towards cattle youngstock rearing and disease, Livestock 25(6): 274-281.
- Love WJ, Lehenbauer TW, Van Eenennaam AL, Drake CM, Kass PH, Farver TB and Aly SS (2016). Sensitivity and specificity of on-farm scoring systems and nasal culture to detect bovine respiratory disease complex in preweaned dairy calves, Journal of Veterinary Diagnostic Investigation 28(2): 119-128. 7.
- Debbink B (2021). Routine thoracic ultrasound: your gateway to calf consults and practice profits, American Association of Bovine Practitioners 54th Annual Conference Proceedings: 173-174.
- Jourquin S, Lowie T, Bokma J and Pardon B (2024). Accuracy and inter-rater agreement among practitioners using quick thoracic ultrasonography to diagnose calf pneumonia, Veterinary Record 194(7): e3896.
- Puig A, Ruiz M, Bassols M, Fraile L and Armengol R (2022). Technological tools for the early detection of bovine respiratory disease in farms, Animals (Basel) 12(19): 2,623.
- Binversie ES, Ruegg PL, Combs DK and Ollivett TL (2020). Randomized clinical trial to assess the effect of antibiotic therapy on health and growth of preweaned dairy calves diagnosed with respiratory disease using respiratory scoring and lung ultrasound, Journal of Dairy Science 103(12): 11,723-11,735.
Meet the authors
Phil Elkins
Job Title